Corrective Surgery
Surgery remains an important option to consider when dealing with pectus deformities but should always be considered carefully having discussed the pectus problem with a surgeon experienced in performing all types of pectus surgery and ideally is familiar with other forms of treatment.
Surgery may be offered for both pectus excavatum and carinatum, though increasingly non-surgical external compression bracing is becoming the first line treatment for pectus carinatum in younger patients. Prosthetic implants are a type of minor surgery that may be offered in patients with pectus excavatum who are symptom free or wish to avoid a more invasive corrective surgical option. The Vacuum bell, a non-surgical option to ‘suck’ the breast bone or sternum forward is a device worn over time and may improve the pectus excavatum particularly in young patients but it’s long term results remain unclear. Occasionally, patients may be candidates for ‘hybrid’ procedures, where several options are offered to get the desired result.
The choice of which operation depends on type and severity of pectus deformity, and the operation that is likely to offer the best functional and cosmetic result as well as considering the risks involved.
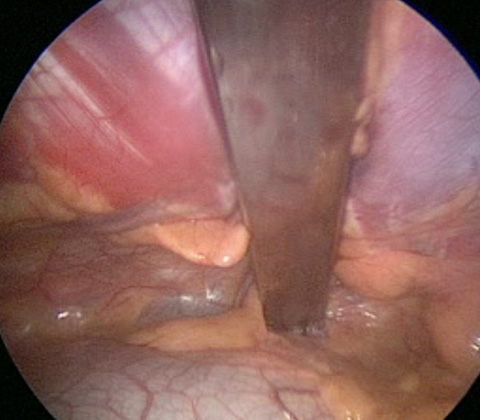
Intraoperative image of bar in place at deepest point of pectus excavatum lifting and correcting chest deformity
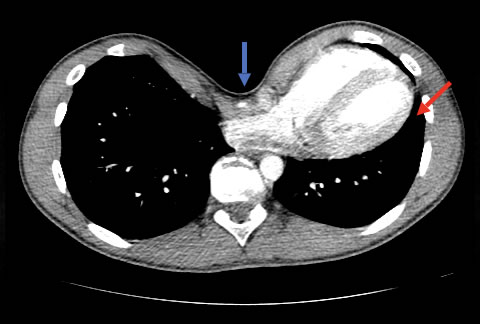
Chest CT showing significant sternal depression (blue arrow) of the heart and left lung (red arrow)
Please click on the buttons below to see and read about patients verified experiences (in their own words) and testimonials (which generally include before and after treatment photos). The pectus clinic is very grateful to all the patients who provided feedback.
Patient selection
The decision to have surgical correction is largely based on the severity and type of pectus deformity, patient choice including the psychosocial impact and physical or functional issues. In patients with symptoms, further investigations should be considered to identify patients with pectus associated functional impairment including musculoskeletal issues. In addition, relative contraindications to surgical correction include complex congenital heart and lung problems and neurodevelopmental disorders.
In the UK across the country about 300 pectus operations are performed each year. Though the trend is toward NUSS procedures, still more open operations are being performed, mainly for pectus excavatum, and this is likely to reflect local surgical experience.
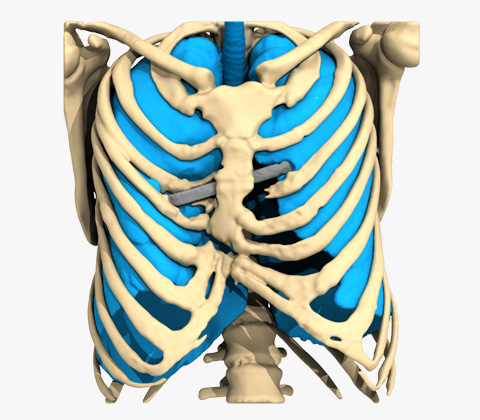
Created for Pectus Clinic by AntomikModeling.
Reconstruction on a patient who had a Modified Ravitch previously.
Patient choice
Patients will often seek an expert opinion to understand more about the underlying pectus deformity and its effect on the body including symptoms that they may have, as well as how it appears. Unfortunately, they may have received little or no information, advice or appreciation of what a pectus deformity is previously. In young patients, it is important to elucidate the patient’s wishes as opposed to those of their parents. It is also essential to consider whether patients require psychological or psychiatric support prior to consideration of correction where there are worrying signs of anxiety, depression or body dysmorphia (a condition where a person spends a lot of time worrying about flaws in their appearance).
Created for Pectus Clinic by AntomikModeling.
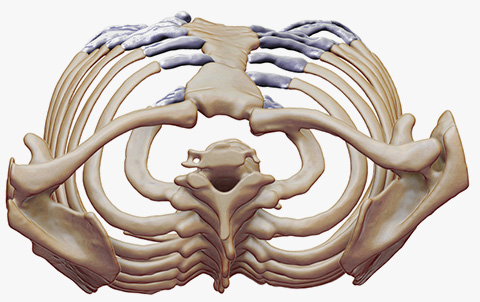
Severe asymmetric pectus carinatum causing significant distortion of the rib cage and sternum
Assessment before surgery
All patients need to be carefully assessed for symptoms and severity of the pectus deformity. Their psychological concerns should be addressed. If symptoms are significant they should be investigated appropriately. Detailed radiology may help the surgeon assess further particularly if severe, asymmetric or a more complex deformity.
Tests (see table below) that may be required before corrective surgery for pectus excavatum. In general, radiology investigations may be all that is required prior to corrective surgery for pectus carinatum unless patient has specific symptoms or concerns.
| Indication | Investigation before corrective surgery |
|---|---|
| All | Chest wall measurements, Medical photography and/or 3D body scan |
| Chest CT or MRI to assess severity and associated features such as sternal rotation as well as calculation of HI and CI | |
| In Presence of Symptoms: | |
| Breathlessness | Lung function tests. Consider CPET |
| Palpitations, syncope or pre-syncope | ECG, Transthoracic echocardiogram. Consider Stress Echocardiogram |
| Significant Psychological features | Psychological assessment |
| Features of Marfan syndrome | Chest CT, Transthoracic echocardiogram, genetic referral for Fibrillin-1 mutation and ophthalmology review |
| Those undergoing Bar insertion including Nuss procedure | Metal allergy testing (titanium bars can be considered if there is a metal allergy) |
Surgery for Pectus Excavatum
Surgical correction of the underlying chest wall deformity can be performed through internally bracing the sternum forward, called the Nuss procedure or Minimally Invasive Repair of Pectus Excavatum (MIRPE). Alternatively, the sternum can be brought forward through a ‘break and re-set’ of the chest wall, known as a Modified Ravitch procedure. Both remain important options in treating pectus excavatum particularly in the context of physical or functional problems.


Severe pectus excavatum before (left) & after a Nuss procedure (right)
Severity
Whilst many patients may be offered surgery on the basis of a clinical assessment of severity of the deformity, the severity can also be quantified by calculating the Haller index (HI). This is a comparison of the width of the thoracic cavity to the depth between the sternum and spine on computer tomography (CT). Alternatives to a CT now include a rapid MRI (magnetic resonance imaging) protocol and 3D topographic body scanning which minimise the radiation exposure in this young patient population.
Typically, a Haller index of >3.25 is considered an indication for surgery, however, this may be helped by a correction index (CI) which accounts for abnormal chest shapes. The CI unlike the HI which relies on the width of the chest wall, appears more accurate in non-standard chest shapes such as an asymmetric chest. A CI >28% correlates with a Haller Index of >3.25.
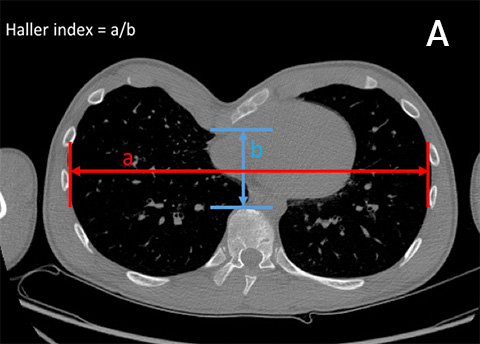
Image of CT scan of a pectus patient showing: (A) Haller index, a measurement of the internal transverse diameter of the thorax on the inside of the rib cage (in red), divided by the shortest anteroposterior depth from the internal aspect of the sternum of the anterior cortex of the nearest vertebral body (in blue)
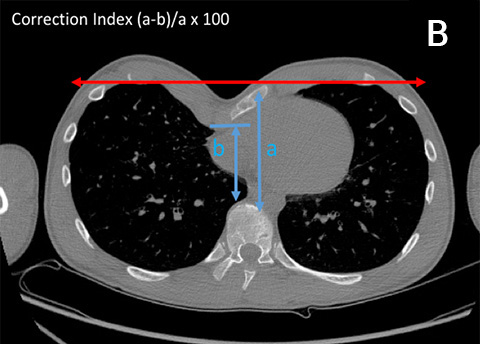
Image of CT scan of a pectus patient showing: (B) Corrective Index is the ratio of the anticipated rise in the sternal defect (in red) after bar placement (a), to the shortest anteroposterior dimension of the inner chest (b), multiplied by 100. It does not rely on the transverse diameter of the chest
Functional impairment
Compression of structures in the chest secondary to the deformity can cause a decrease in internal chest volume and can lead to heart and lung impingement. It is suggested that symptoms may worsen with age, but the significance of the functional or physical effects of pectus excavatum is controversial and remains an important topic of debate.
Lung Function tests
Lung or pulmonary function tests (PFTs) are regularly performed to investigate exertional breathlessness, ‘wheeziness’ or associated respiratory problems in patients with pectus deformity. However, they are often difficult to interpret, and can appear normal or ‘near normal’. With very severe pectus excavatum, the lungs may be restricted by its compressive effect. In addition, recent research has examined how pectus affects chest wall movement and whether it affects breathing and importantly the sensation of breathlessness particularly during exercise.
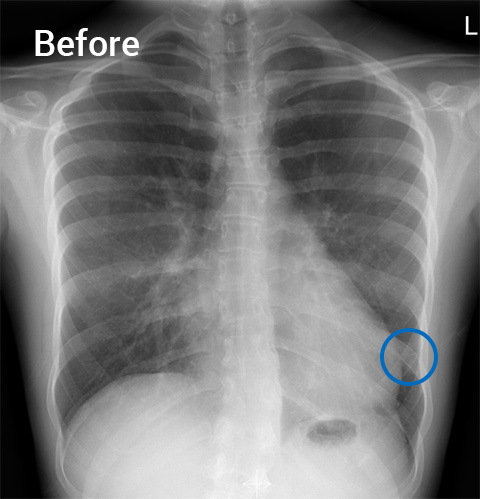

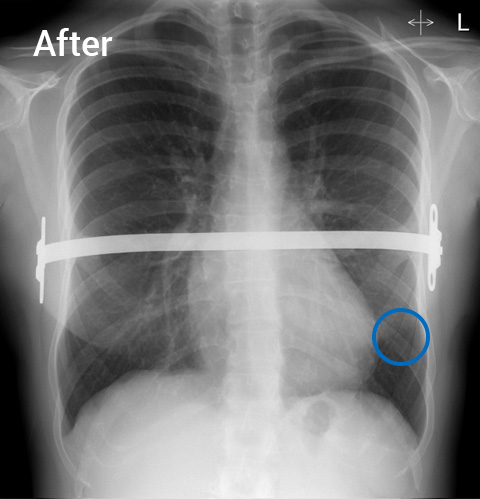
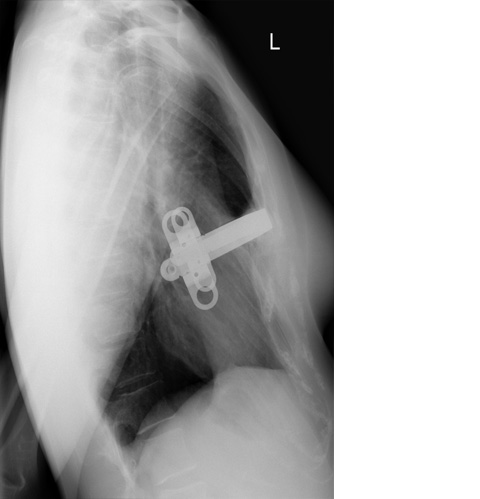
Before (left) and 3 years after (right) a Nuss procedure with front and side X-ray views showing changing in position of the heart and lungs from an abnormal left sided heart shadow and compression of left lung to a normal central heart position (After) (highlighted by the blue rings).
Heart Function
The effect of sternal displacement pushing backwards particularly in severe pectus excavatum is obvious physically, on X-ray and on the echocardiogram (heart ultrasound scan). Patients often complain of a ‘constrictive’ feeling and palpations. In severe cases, it causes cardiac compression, and especially affects the right heart. However, like lung function, data from studies remains contradictory and with no consensus on whether the heart is significantly affected despite patient symptoms.
Video: Cardiac MRI demonstrating significant cardiac compressive
Choice of operation
The two most common types of corrective surgical repair of pectus excavatum are the MIRPE (Minimally Invasive Repair of Pectus Excavatum) or Nuss procedure and the ‘open’ Modified Ravitch operation. The choice of procedure depends on factors including age of patient, severity of deformity, associated significant asymmetry and sternal rotation, risk of complications and the experience of the surgical team.

Nuss procedure
The Nuss or MIRPE operation is a keyhole operation involving insertion of a metal bar behind the breastbone to correct the pectus excavatum.

Modified Ravitch operation
The Modified Ravitch procedure is a ‘Open’ operation involving essentially breaking and re-setting the front of the rib cage and breastbone to correct the pectus excavatum.
Surgery for Pectus Carinatum
For surgical correction of pectus carinatum the options include a ‘keyhole’ approach or an ’open’ approach. Experienced Pectus surgeons recognise they can be more challenging in terms of achieving a good cosmetic result. In certain selected cases, a ‘hybrid’ option combining surgery and external compressive bracing may offer an less invasive option.
In addition, unlike Pectus excavatum there is much less evidence of pectus carinatum causing physical symptoms leading to a functional or physiological problem though the psychological impact should not be underestimated.

Severe pectus carinatum before surgery
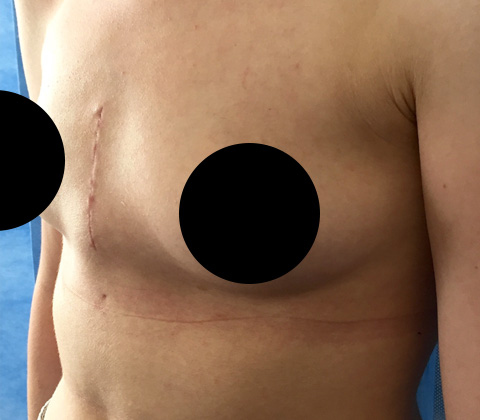
After a Modified Ravitch procedure in the same patient
Severity
Unlike pectus excavatum, the severity of the pectus carinatum is often a clinical one and is based on the surgeon’s experience. There are few established radiological assessment tools, though the Pectus Clinic has developed one such tool using topographical measurements. Called, the ’Pectus Index’, a reverse Haller Index, it allows an objective measurement to assess severity of the pigeon chest.
Presentation: Our research was recently presented at the Society of Cardiothoracic Surgeons (SCTS) meeting in Glasgow
Functional impairment
There is no compression of structures in the chest caused by pectus carinatum. Though symptoms, particularly pain and breathlessness on exercise may be noted, the cause of these symptoms is not clear. Like pectus excavatum, such symptoms may be related to how the chest wall movements are affected particularly when breathing heavily. In general, pectus carinatum is not associated with a function problem, though musculoskeletal issues such as ‘stooped or rounded’ shoulders are often seen and can be severe.
Choice of operation
The types of corrective surgical repair of pectus carinatum are the ‘open’ Modified Ravitch operation and less commonly a ‘keyhole’ or Minimally Invasive surgery (MIS) operation, such as the Abrahamson’s technique. In addition, several alternative ’keyhole’ procedures are described including MIS with limited cutting of the cartilage combined with a external compressive brace (a hybrid operation). The choice of procedure depends on factors including age of patient, severity of deformity, associated significant asymmetry and sternal rotation, flexibility of chest wall, risk of complications and the experience of the surgical team.
Modified Ravitch operation
The Modified Ravitch procedure is a ‘Open’ operation involving essentially breaking and re-setting the front of the rib cage and breastbone to correct the pectus carinatum.

Hybrid surgery
In selected cases using a combination of MIS and a subsequent external compression brace worn following surgery can avoid more invasive surgery.
Gallery
We take numerous measurements and photos before, during and after Corrective Surgery treatment as many of the problems we see centre around appearance. With the patient's permission we are happy to share our outcomes.
Results
It is important that we can show evidence that the Corrective Surgery treatment we offer and the results that we achieve are proven. We actively collect data to allow us to study, research and publish are outcomes.
Please click on the buttons below to see and read about patients verified experiences (in their own words) and testimonials (which generally include before and after treatment photos). The pectus clinic is very grateful to all the patients who provided feedback.